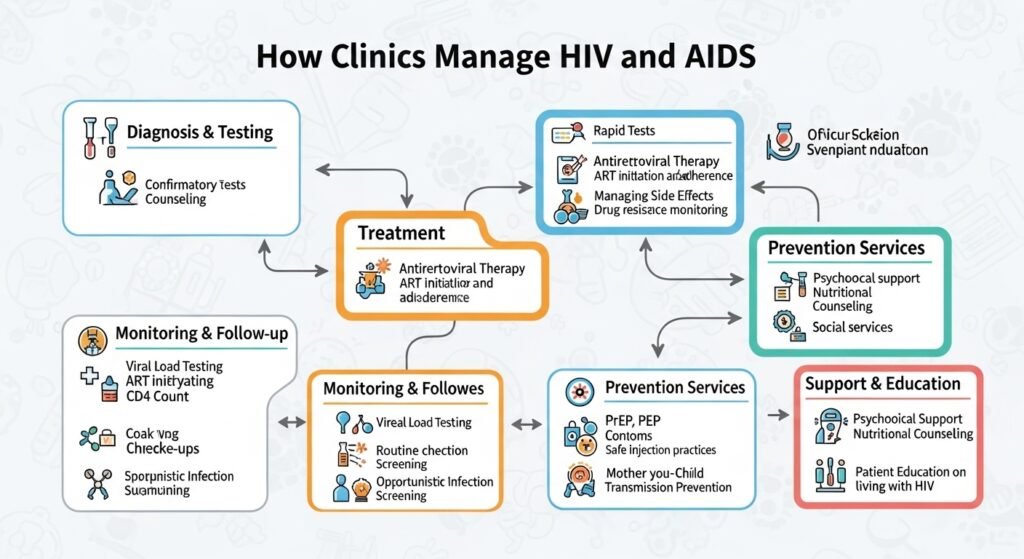
HIV (human immunodeficiency virus) — once a uniformly fatal diagnosis — has been transformed into a manageable chronic condition by antiretroviral therapy (ART). People with HIV who are diagnosed early and adherent to treatment can expect near-normal life expectancy. Medical clinics — both primary care practices and dedicated HIV clinics — provide the comprehensive, long-term care that achieves this outcome. This guide explains how clinics manage HIV and support the health of people living with HIV.
HIV Testing: The First Step
The CDC recommends HIV testing for all Americans aged 13–64 at least once, and annually for those with ongoing risk factors (multiple partners, injectable drug use, sex work). Clinics provide confidential HIV testing through blood tests (4th generation combination antigen/antibody tests that detect HIV within 18–45 days of infection) and self-test kits available for home use.
Antiretroviral Therapy
ART combines multiple medications from different drug classes to suppress HIV viral replication to undetectable levels. When viral load is undetectable, CD4 count (immune cells) stabilizes or recovers, and the person cannot transmit HIV to partners (Undetectable = Untransmittable, U=U). Modern ART regimens — many available as once-daily single pills — are well-tolerated and highly effective. Starting ART promptly after diagnosis, regardless of CD4 count, is the current standard of care.
HIV Prevention
PrEP (pre-exposure prophylaxis) — daily oral medication (tenofovir/emtricitabine or cabotegravir injection) — reduces HIV transmission risk by over 99% in adherent individuals. Clinics prescribe and monitor PrEP for HIV-negative individuals at ongoing risk of HIV exposure. PEP (post-exposure prophylaxis) — a 28-day ART course started within 72 hours of a potential exposure — prevents HIV infection after potential exposure.
Conclusion
HIV is now a manageable chronic condition — the transformation in outcomes over the past three decades is one of medicine’s greatest achievements. Know your HIV status, access testing through your clinic, start treatment promptly if diagnosed, and if at ongoing risk, discuss PrEP with your healthcare provider. The goal of ending the HIV epidemic is achievable through testing, treatment, and prevention.
FAQs – HIV and AIDS Clinic Management
Q1. What is the difference between HIV and AIDS?
A: HIV is the virus; AIDS is the late stage of HIV infection, defined by CD4 count below 200 cells/mm³ or development of an AIDS-defining opportunistic infection. With effective ART, progression from HIV to AIDS is preventable.
Q2. Can HIV be cured?
A: No broadly applicable cure currently exists. A small number of patients have been effectively cured through bone marrow transplants using HIV-resistant donor cells, but this approach is not feasible for broad use. Research continues toward functional cure strategies.
Q3. Is HIV only transmitted through sexual contact?
A: HIV transmits through specific bodily fluids: blood, semen, vaginal fluids, rectal fluids, and breast milk. Routes include sexual contact, shared injection equipment, and mother-to-child transmission during pregnancy, birth, or breastfeeding. It is not transmitted through casual contact.
Q4. Does HIV treatment affect quality of life?
A: Modern ART regimens are far better tolerated than older medications. Most people starting current ART experience minimal side effects. Some long-term side effects (metabolic, cardiovascular, bone effects) are monitored through regular clinic visits.
Q5. How often should a person with HIV see their doctor?
A: When starting ART or changing regimen, every 1–3 months until stable. When established on effective therapy with stable health, every 3–6 months. CD4 count, viral load, and comprehensive metabolic monitoring are performed at each visit.


