Benign prostatic hyperplasia (BPH) — non-cancerous enlargement of the prostate gland — is one of the most common conditions affecting older men, with prevalence increasing from 50% of men in their 50s to over 80% in their 70s and 80s. As the prostate grows, it compresses the urethra, causing lower urinary tract symptoms (LUTS) that significantly affect quality of life. Urology and primary care clinics evaluate and manage BPH across a spectrum from watchful waiting to medication to minimally invasive procedures. This guide explains BPH care.
Symptoms
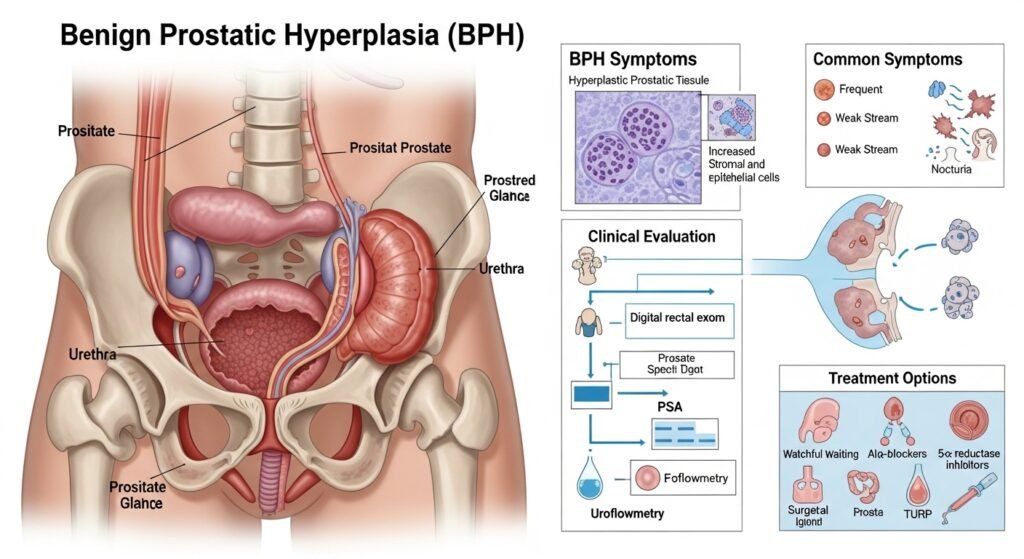
BPH causes obstructive symptoms (weakened urinary stream, difficulty starting urination, incomplete bladder emptying, urinary hesitancy, dribbling after urination) and irritative symptoms (urgency, frequency, nocturia — waking multiple times at night to urinate). The International Prostate Symptom Score (IPSS) quantifies symptom severity and guides treatment decisions. BPH symptoms alone do not indicate prostate cancer — distinguishing benign from malignant prostate disease requires PSA testing and digital rectal examination.
Medical Treatment
Alpha-blockers (tamsulosin, alfuzosin) relax smooth muscle in the prostate and bladder neck, improving urine flow within days. 5-alpha reductase inhibitors (finasteride, dutasteride) reduce prostate volume over months, best suited for men with significantly enlarged glands. Combination therapy provides superior symptom control for men with both large prostate size and significant obstructive symptoms. Phosphodiesterase-5 inhibitors (tadalafil) are approved for both BPH and erectile dysfunction.
Minimally Invasive and Surgical Procedures
For men with severe symptoms or inadequate medication response, options include: UroLift (implants that hold prostatic lobes apart without tissue removal), Rezūm (water vapor thermal therapy that destroys excess prostate tissue), and TURP (transurethral resection of the prostate — the gold standard surgical procedure for BPH).
Conclusion
BPH is common and effectively manageable through your urology or primary care clinic. Do not normalize urinary symptoms as “just part of aging” — effective treatment significantly improves quality of life. Importantly, ensure that PSA testing is conducted alongside BPH evaluation to appropriately evaluate for prostate cancer.
FAQs – BPH
Q1. Does BPH cause prostate cancer?
A: No. BPH is entirely separate from prostate cancer — it does not cause, transform into, or increase risk of prostate cancer. However, both BPH and prostate cancer can cause similar urinary symptoms, and both may be present simultaneously, requiring evaluation to distinguish them.
Q2. Does BPH affect sexual function?
A: BPH itself can contribute to erectile dysfunction through shared mechanisms. Some BPH medications (5-alpha reductase inhibitors) can reduce libido and erectile function. Alpha-blockers generally do not affect erectile function and may improve it in some patients.
Q3. How is BPH diagnosed?
A: Diagnosis is based on history (symptom assessment using IPSS), physical examination including digital rectal exam, urinalysis to exclude infection, and PSA testing to assess prostate cancer risk. Urodynamic testing or cystoscopy may be performed for complex presentations.
Q4. Can diet affect BPH?
A: Some evidence suggests that diets low in red meat and high in vegetables may reduce BPH progression. Reducing fluid intake in the evening (to reduce nocturia) and limiting caffeine and alcohol are practical dietary modifications that reduce symptom severity.
Q5. What happens if BPH is untreated?
A: Severe untreated BPH can cause urinary retention (complete inability to urinate — a medical emergency), recurrent urinary tract infections, bladder stones, and over time, bladder muscle weakening from chronic obstruction and kidney damage from back-pressure on the collecting system.


