Sepsis — the body’s life-threatening response to infection, in which the immune response damages its own tissues and organs — kills approximately 270,000 Americans annually, making it one of the leading causes of preventable hospital deaths. Early recognition and rapid treatment dramatically improve survival — survival rates decline by approximately 7% for each hour of delay in appropriate treatment. Medical clinics play a critical role in recognizing sepsis early — before patients deteriorate to septic shock — and initiating or expediting treatment. This guide explains sepsis recognition and response at the clinic level.
Recognizing Sepsis
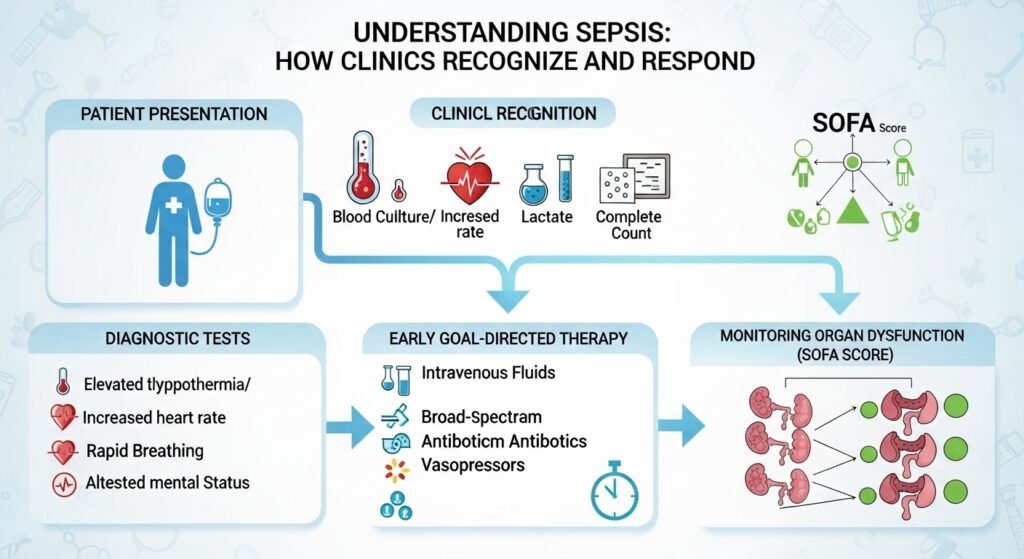
Sepsis should be suspected in any patient with known or suspected infection who exhibits: fever (above 38.3°C/101°F) or hypothermia (below 36°C/96.8°F), tachycardia (heart rate above 90 bpm), tachypnea (respiratory rate above 22 breaths/min), altered mental status, or signs of organ dysfunction. The qSOFA criteria provide a simple bedside screen: respiratory rate ≥22, altered mental status, and systolic BP ≤100 mmHg — two of three positives identify high-risk patients. Important: elderly and immunocompromised patients may not mount a fever despite serious infection — absence of fever does not exclude sepsis.
Clinic Response
Clinics are not equipped to manage established sepsis requiring intensive organ support — the appropriate clinical action is immediate emergency services activation and hospital transfer. Clinics can: recognize sepsis early through systematic assessment of vital signs and clinical status; initiate blood cultures and preliminary workup; administer a fluid bolus and initial antibiotics when transfer is anticipated to be delayed; and provide the emergency responders with the clinical assessment that accelerates in-hospital management.
The Sepsis “Bundle”
Hospital management of sepsis follows the Surviving Sepsis Campaign bundle: blood cultures before antibiotics, broad-spectrum antibiotics within one hour of sepsis recognition, fluid resuscitation for hypotension or elevated lactate, vasopressors for persistent hypotension, and lactate measurement to identify tissue hypoperfusion. Each component of this bundle, implemented within 1 hour, saves lives.
Conclusion
Sepsis is a medical emergency — time to antibiotics is one of the most critical determinants of outcome. If a clinic patient appears seriously ill with infection, immediate vital sign assessment, sepsis screening, and emergency transfer preparation is the appropriate response. Telling family members and patients to watch for sepsis warning signs during management of serious infections — and to call 911 if they develop worsening symptoms, confusion, or extreme weakness — enables earlier community recognition of this life-threatening complication.
FAQs – Sepsis
Q1. What infections most commonly cause sepsis?
A: Pneumonia is the most common source, followed by abdominal infections (appendicitis, diverticulitis, biliary sepsis), urinary tract infections (urosepsis), and skin/soft tissue infections. Blood stream infections (bacteremia) without a localizing source also occur.
Q2. What is septic shock?
A: Septic shock is the most severe form of sepsis — characterized by sepsis plus persistent hypotension despite adequate fluid resuscitation, and elevated lactate indicating cellular oxygen delivery failure. Septic shock mortality is 40–50% even with aggressive treatment.
Q3. Can a UTI cause sepsis?
A: Yes. Urosepsis — sepsis from urinary tract infection — is common, particularly in elderly patients, those with urinary tract abnormalities, and immunocompromised individuals. Prompt antibiotic treatment of UTI prevents progression to urosepsis.
Q4. How do I know if I or someone I know has sepsis?
A: Warning signs of sepsis include: extreme shivering or feeling very cold; skin that is pale, mottled, or has unusual color; a rash that doesn’t fade when pressed; high or very low temperature; rapid breathing; feeling confused or disoriented; and feeling extremely unwell. SEPSIS is remembered by the mnemonic S-E-P-S-I-S: Slurred speech or confusion, Extreme shivering, Passing no urine, Severe breathlessness, It feels like you might die, Skin mottled or discolored. Call 911 if you suspect sepsis.
Q5. Can sepsis be prevented?
A: Sepsis prevention includes: vaccination (reduces infections that cause sepsis — particularly pneumococcal and influenza), prompt treatment of infections before they progress, good wound care, hand hygiene in healthcare settings, and appropriate antibiotic stewardship to prevent resistant organisms. Complete prescribed antibiotic courses for known infections to prevent treatment failure that allows sepsis development.


