Shortness of breath (dyspnea) — the uncomfortable awareness of difficult breathing — is one of the most common and potentially serious symptoms prompting clinic visits. Like chest pain, dyspnea has an enormously broad differential diagnosis ranging from deconditioning and anxiety to heart failure, pulmonary embolism, and severe pneumonia. Appropriate clinical assessment rapidly triages patients to emergency care, urgent specialist evaluation, or further outpatient workup based on severity, acuity, and associated features. This guide explains clinical dyspnea evaluation.
When Shortness of Breath Is an Emergency
Call 911 for: sudden severe dyspnea at rest; dyspnea with chest pain; dyspnea with reduced consciousness or inability to speak in complete sentences; cyanosis (blue lips or fingertips); rapid deterioration in breathing; stridor (high-pitched sound with inspiration suggesting upper airway obstruction); and any patient in severe respiratory distress. These presentations require emergency airway management, supplemental oxygen, and definitive treatment available only in an emergency setting.
Common Causes and Distinguishing Features
Cardiac causes (heart failure, acute coronary syndrome) — orthopnea (worsened lying flat), paroxysmal nocturnal dyspnea, leg edema, history of cardiac disease. Pulmonary causes (asthma, COPD, pneumonia, pneumothorax, PE) — wheezing (airway obstruction), pleuritic chest pain (pneumonia, PE), fever, sudden onset in a young person without prior lung disease. Anemia — progressive dyspnea on exertion with fatigue. Deconditioning — dyspnea only with significant exertion. Anxiety — dyspnea with other anxiety symptoms, often accompanied by tingling extremities and chest tightness.
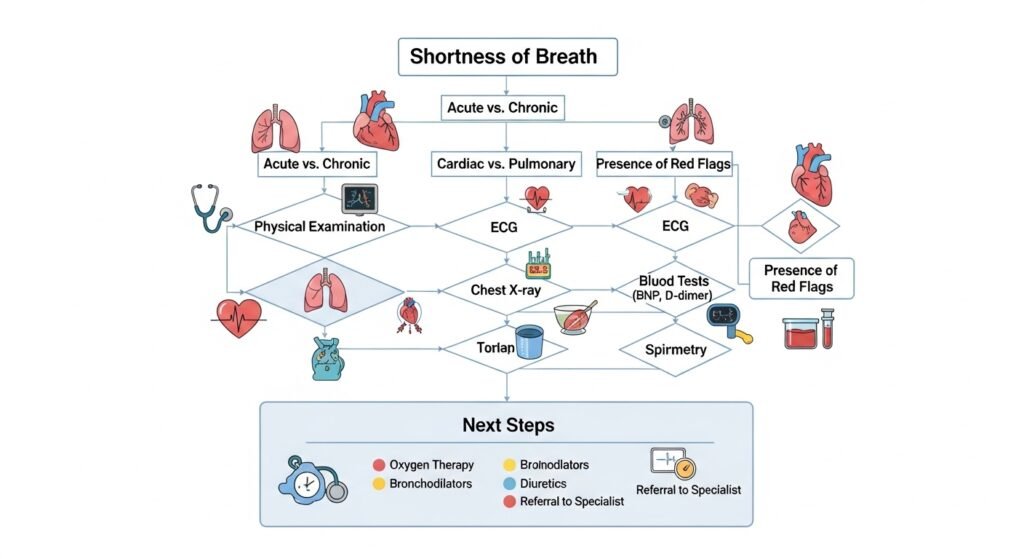
Clinic Assessment
Vital signs — oxygen saturation (SpO2) on room air is the most important initial vital sign in dyspnea evaluation. SpO2 below 90% indicates significant hypoxia requiring oxygen supplementation and urgent evaluation. Chest auscultation identifies wheezing, crackles, absent breath sounds. ECG assesses for cardiac arrhythmia and ischemia. Chest X-ray evaluates for pneumonia, pneumothorax, effusion, and cardiomegaly. BNP assesses heart failure. CBC identifies anemia. Spirometry evaluates airflow obstruction.
Conclusion
Shortness of breath always deserves evaluation — the body’s oxygen delivery system is too fundamental to ignore. Severity, acuity, associated symptoms, and oxygen saturation guide whether emergency or outpatient evaluation is appropriate. When in doubt about a patient who is struggling to breathe, emergency evaluation is the safer choice. For chronic or progressive dyspnea with normal oxygen saturation, structured clinic evaluation identifies the cause and guides appropriate management.
FAQs – Shortness of Breath
Q1. What does a normal oxygen saturation level look like?
A: Normal SpO2 is 95–100%. Readings of 90–94% indicate mild to moderate hypoxia requiring evaluation. Below 90% indicates significant hypoxia — supplemental oxygen is indicated and emergency evaluation is warranted. Readings may be inaccurate with nail polish, poor perfusion, and certain hemoglobin variants (including carboxyhemoglobin in CO poisoning).
Q2. Can anxiety cause shortness of breath?
A: Yes. Anxiety triggers hyperventilation — rapid, shallow breathing that lowers carbon dioxide levels, causing respiratory alkalosis, which produces numbness and tingling in extremities, lightheadedness, and paradoxically, increased sensation of breathlessness. Anxiety-related breathing retraining can help manage this pattern.
Q3. What is orthopnea and what causes it?
A: Orthopnea is dyspnea that worsens when lying flat and improves when sitting or standing upright. It is characteristic of heart failure — in the supine position, fluid redistributes from the legs to the lungs, increasing pulmonary venous pressure and worsening breathlessness. The number of pillows needed to sleep comfortably provides a rough measure of severity.
Q4. Can being out of shape cause shortness of breath?
A: Yes. Deconditioning causes dyspnea on exertion as the cardiovascular system cannot meet the oxygen demand of exercise efficiently. However, deconditioning is a diagnosis of exclusion — other causes should be considered and evaluated before attributing dyspnea solely to fitness level, particularly when dyspnea is new or progressive.
Q5. What is pulmonary embolism and should I worry about it?
A: Pulmonary embolism (PE) — a blood clot in the pulmonary arteries — causes sudden shortness of breath, sometimes with pleuritic chest pain and hemoptysis (coughing blood). Risk factors include prolonged immobility (long flight, bedrest), recent surgery, cancer, pregnancy, and prior clotting disorders. PE requires urgent evaluation with CT pulmonary angiography and anticoagulation treatment. It is genuinely life-threatening — suspicion of PE warrants emergency evaluation.


