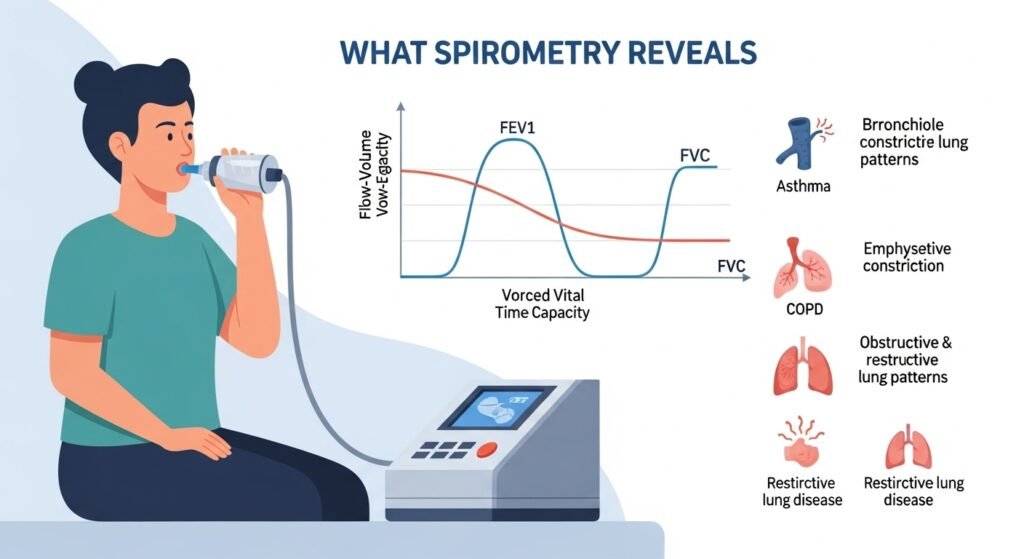
Spirometry is the primary clinical test of lung function — a simple, inexpensive breathing test that measures how much air the lungs can hold and how fast air can be expelled. It is essential for diagnosing and monitoring obstructive (COPD, asthma) and restrictive (pulmonary fibrosis, chest wall disorders) lung diseases, assessing pre-operative respiratory risk, and monitoring the effects of treatment on lung function over time. Medical and pulmonary clinics perform spirometry routinely. This guide explains what spirometry measures and how results are interpreted.
Key Spirometric Measurements
FVC (forced vital capacity) — the total amount of air exhaled forcefully after maximum inhalation. FEV1 (forced expiratory volume in 1 second) — the amount expelled in the first second. FEV1/FVC ratio — the proportion of FVC expelled in the first second. A normal FEV1/FVC above 0.70 indicates no significant obstruction. Below 0.70 confirms obstructive airway disease (COPD or asthma). Reduced FVC with preserved or elevated FEV1/FVC indicates a restrictive pattern.
How the Test Is Performed
You take a maximum breath, then blow out as hard and fast as possible through a mouthpiece connected to a spirometer — holding the effort for at least 6 seconds. The test is repeated at least three times to ensure reproducibility. A bronchodilator (albuterol inhaler) is administered and spirometry repeated after 10–15 minutes to assess reversibility — a hallmark of asthma versus COPD.
What Results Mean
Normal spirometry makes significant obstructive lung disease unlikely (though not impossible in early disease). Obstructive pattern with reversibility suggests asthma. Obstructive pattern without significant reversibility, combined with appropriate history, confirms COPD. Restrictive pattern prompts further evaluation with full pulmonary function testing (including lung volumes and diffusing capacity).
Conclusion
Spirometry is an underutilized, invaluable diagnostic tool — it takes 15 minutes, requires no needles or radiation, and provides quantitative information about lung function that guides the diagnosis and management of the most common respiratory conditions. Any patient with unexplained breathlessness, chronic cough, or significant smoking history should have spirometry performed.
FAQs – Spirometry
Q1. Does spirometry hurt?
A: No. The test requires forceful breathing effort but causes no pain. Some patients feel slightly lightheaded or dizzy after the forced exhalation maneuvers — this resolves quickly with rest.
Q2. Can I take my inhalers before spirometry?
A: For diagnostic spirometry, you are typically asked to withhold short-acting bronchodilators for 4–6 hours and long-acting bronchodilators for 12–24 hours before the test, so that baseline (pre-bronchodilator) function can be measured. Follow your clinic’s specific instructions.
Q3. How often should spirometry be performed for COPD patients?
A: Annual spirometry is recommended for COPD patients to monitor disease progression and treatment response. More frequent testing is performed when symptoms change significantly or treatment adjustments are being evaluated.
Q4. What is a full pulmonary function test (PFT)?
A: A comprehensive PFT panel adds lung volume measurements (functional residual capacity, total lung capacity, residual volume) and diffusing capacity (DLCO — measuring gas exchange efficiency) to spirometry. Full PFTs characterize restrictive diseases and assess emphysema severity in COPD.
Q5. Is spirometry the same as the “breath test” for H. pylori?
A: No. The urea breath test for H. pylori (the bacterium causing stomach ulcers) is a completely different test using isotope-labeled urea. Spirometry measures airflow; the urea breath test detects H. pylori enzymatic activity. The only similarity is that both involve breathing into a device.