Falls are the leading cause of injury death in Americans over 65, causing over 36,000 deaths annually and resulting in 3 million emergency department visits. Hip fractures — the most devastating fall consequence — are associated with a 20–30% one-year mortality rate and loss of independent living in many survivors. Medical clinics play a critical preventive role in identifying fall risk, addressing modifiable factors, and implementing evidence-based interventions that reduce falls and their consequences. This guide explains how clinics approach fall prevention in older adults.
Fall Risk Assessment
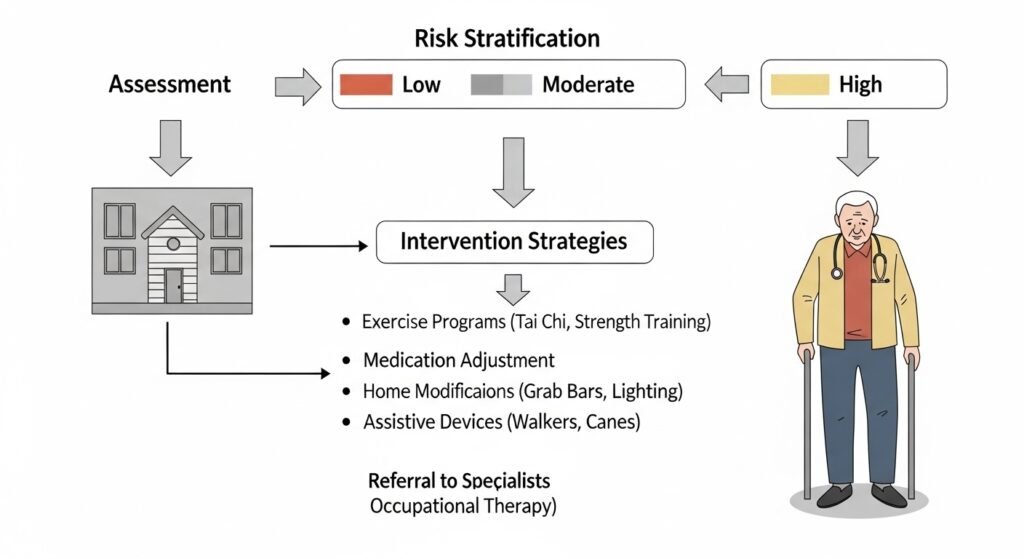
Clinics screen older adults for fall risk annually using tools including: single question screening (“Have you fallen in the past year?”), Timed Up and Go test (measuring time to stand from a chair, walk 10 feet, turn, return, and sit — over 12 seconds indicates elevated fall risk), and comprehensive balance and gait assessment. Identifying patients at elevated fall risk triggers a more detailed multi-factorial evaluation.
Modifiable Fall Risk Factors
- Polypharmacy and specific medications (benzodiazepines, sleep aids, anticholinergics, antihypertensives) — medication review and deprescribing
- Orthostatic hypotension — blood pressure drops with position change
- Vision impairment — annual eye exams and corrective lenses
- Foot problems — appropriate footwear, podiatry care
- Home hazards — throw rugs, poor lighting, no grab bars
- Muscle weakness and balance impairment — addressed through physical therapy
- Vitamin D deficiency — supplementation reduces fall risk
Interventions
Exercise programs targeting strength and balance (tai chi, matter of balance programs) consistently reduce fall rates by 21–39% in clinical trials. Physical therapy provides individualized balance training. Occupational therapy conducts home safety assessments and recommends modifications (grab bars, improved lighting, stair rails). Medication review eliminates or replaces high-fall-risk medications.
Conclusion
Falls are preventable — not an inevitable consequence of aging. Systematic fall risk assessment, identification of modifiable risk factors, and evidence-based interventions through primary care and geriatric clinics significantly reduce fall rates and their devastating consequences. If you or a family member has fallen or feels unsteady, bring this to your clinic’s attention as a clinical priority.
FAQs – Fall Prevention
Q1. What medications increase fall risk?
A: Benzodiazepines and sleep aids, anticholinergic medications, opioids, first-generation antihistamines, blood pressure medications causing orthostatic hypotension, and polypharmacy (≥5 medications) collectively represent the highest pharmacological fall risk. Medication review by a pharmacist or geriatrician identifies candidates for deprescribing.
Q2. Does vitamin D deficiency cause falls?
A: Vitamin D deficiency causes muscle weakness and impairs neuromuscular function, contributing to fall risk. Supplementation (800–1,000 IU/day) reduces falls in vitamin D-deficient older adults — particularly those confined to home or with limited sun exposure.
Q3. When should a medical alert device be considered?
A: Any older adult living alone who has fallen or has significant fall risk benefits from a medical alert device enabling immediate emergency call for help. Modern devices include GPS tracking and automatic fall detection in addition to manual emergency buttons.
Q4. How does physical therapy help prevent falls?
A: Physical therapists assess and treat the specific impairments contributing to fall risk — muscle weakness, balance dysfunction, gait abnormalities, and fear of falling. Individualized exercise programs targeting these deficits produce meaningful improvements in balance and fall frequency.
Q5. What should I do if I find a fallen family member?
A: Call 911 if the person is injured, unconscious, or cannot get up safely. Do not attempt to lift them without proper technique — this risks injury to both the fallen person and helper. Assess for injury after the fall and ensure prompt medical evaluation to identify any underlying cause.