Dual-energy X-ray absorptiometry (DEXA) is the gold standard clinical test for measuring bone mineral density (BMD) — the primary diagnostic tool for osteoporosis and osteopenia. Using two low-dose X-ray beams at different energies, DEXA measures how much radiation is absorbed by bone versus soft tissue at specific skeletal sites, providing quantitative BMD data that diagnoses bone loss and assesses fracture risk. This guide explains how DEXA scans work, who should have them, and how results are interpreted.
How DEXA Is Performed
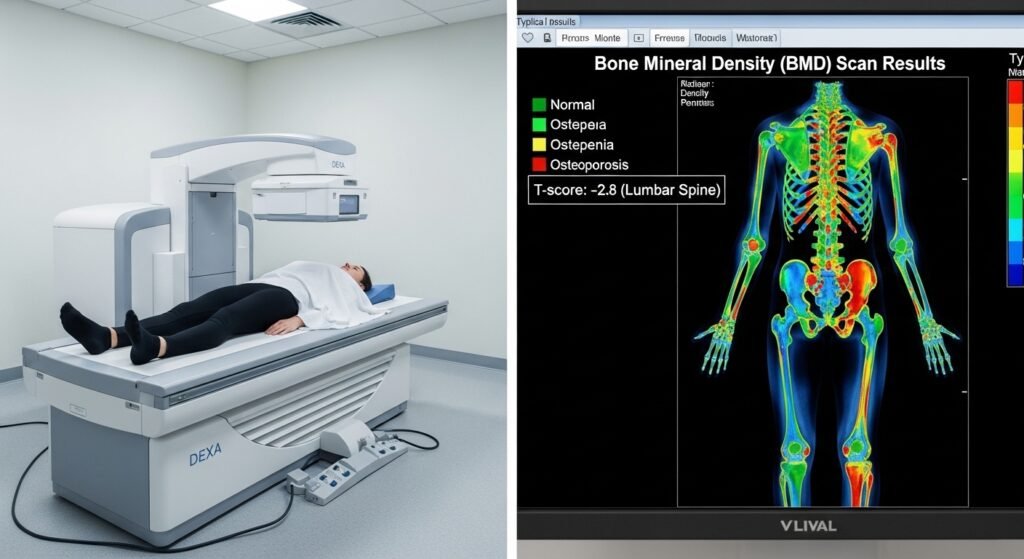
You lie fully clothed on a padded table while a mechanical arm passes over your body, emitting low-dose X-ray beams. The two most important measurement sites are the lumbar spine (L1–L4 vertebrae) and the proximal femur (hip) — the locations most predictive of fracture risk. A forearm scan is added when spine and hip measurements are technically difficult. The entire test takes 10–20 minutes and involves radiation exposure equivalent to a few hours of background radiation — far less than a chest X-ray.
Understanding Your Results
DEXA results are reported as T-scores: the number of standard deviations your BMD falls above or below the average peak bone density of a healthy young adult. T-score above -1.0: normal. -1.0 to -2.5: osteopenia (low bone mass, not yet osteoporosis). Below -2.5: osteoporosis. Z-scores compare BMD to age-matched peers — relevant for premenopausal women, men under 50, and children.
Who Should Have a DEXA Scan
Current recommendations: all women aged 65 and older; younger postmenopausal women with risk factors (fracture history, weight below 57kg, parental hip fracture, current smoking, daily alcohol use, rheumatoid arthritis, long-term steroid use). Men should discuss screening with their doctor at age 70 or earlier if significant risk factors are present.
Conclusion
DEXA scanning is a fast, safe, and definitive test for osteoporosis — one of the most underdiagnosed and undertreated conditions affecting older adults. Know your T-score, discuss fracture risk with your clinic, and implement the lifestyle and pharmacological measures that protect bone density and prevent the fractures that can irreversibly alter independence and quality of life.
FAQs – DEXA Scans
Q1. How accurate is a DEXA scan?
A: DEXA has excellent reproducibility (coefficient of variation typically 1–2%) at the same scanner. BMD values can vary between different scanner models — for longitudinal monitoring, use the same scanner for consistent comparisons.
Q2. Can I eat or drink before a DEXA scan?
A: Yes. No fasting is required. Avoid calcium supplements for 24 hours before the scan — large calcium doses can slightly affect results. Wear comfortable clothing without metal (metal fasteners interfere with measurements).
Q3. How often should DEXA be repeated?
A: For monitoring treatment response, DEXA is typically repeated every 1–2 years. For normal bone density monitoring without treatment, every 2–5 years based on risk level is appropriate. More frequent scanning adds limited information once treatment response is established.
Q4. Can men develop osteoporosis?
A: Yes. Approximately 2 million American men have osteoporosis and 12 million have osteopenia. Men fracture hips less often than women at comparable bone density levels but have higher mortality after hip fracture. Male osteoporosis is underrecognized and undertreated.
Q5. Does DEXA scan show arthritis?
A: Significant spinal arthritis (osteoarthritis with bone spurs) artificially elevates lumbar spine BMD readings, potentially masking true bone density loss. In patients with significant spinal arthritis, the hip measurement is more reliable for fracture risk assessment.