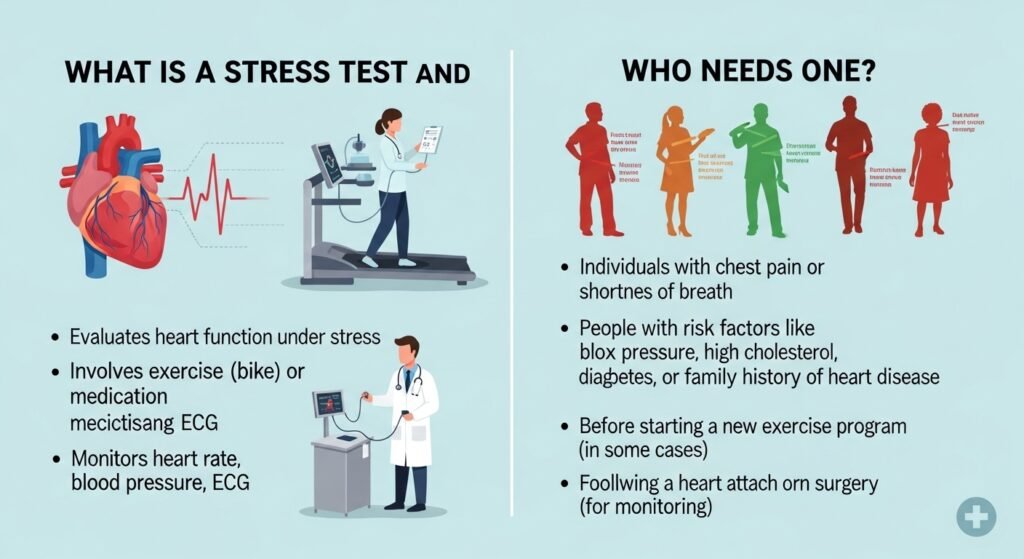
A cardiac stress test — commonly called an exercise stress test or treadmill test — evaluates how the heart performs during physical exertion. Because some heart problems only manifest when the heart is working harder (requiring more blood flow than narrowed coronary arteries can supply at rest), stress testing reveals abnormalities invisible on a resting ECG. Cardiology and primary care clinics order stress tests for a variety of diagnostic and risk-stratification purposes. This guide explains who needs a stress test and what it can detect.
Types of Stress Tests
Exercise ECG Stress Test
The basic stress test — you walk on a treadmill (or pedal a stationary bicycle) while your ECG, blood pressure, and heart rate are continuously monitored. The exercise intensity increases in stages. A positive test (ST-segment changes indicating ischemia, significant arrhythmias, exertional symptoms, or blood pressure drop) suggests significant coronary artery disease requiring further evaluation.
Nuclear Stress Test
A radiotracer injected intravenously shows myocardial perfusion — areas of the heart receiving inadequate blood flow during stress appear as perfusion defects on nuclear imaging. This provides more detailed localization information than ECG alone and is appropriate when the ECG interpretation is unreliable (baseline ECG abnormalities, left bundle branch block, pacemaker).
Stress Echocardiogram
Echocardiographic (ultrasound) images of heart wall motion are obtained at rest and immediately after exercise or pharmacological stress. Regional wall motion abnormalities during stress indicate ischemia in the territory of a narrowed coronary artery.
Pharmacological Stress Test
For patients who cannot exercise adequately, pharmacological agents (dobutamine for echo stress, adenosine or regadenoson for nuclear stress) simulate exercise-like stress on the heart without physical activity.
Who Needs a Stress Test
Stress tests are ordered for evaluation of chest pain or symptoms suspicious for angina, pre-operative cardiac risk assessment before major non-cardiac surgery, evaluation of known or suspected coronary artery disease, assessment of exercise capacity and cardiac function, and evaluation of exercise-induced arrhythmias.
Conclusion
Cardiac stress testing provides important information about coronary artery function that resting tests cannot reveal — detecting significant disease that might otherwise only manifest as a heart attack. If your clinic recommends a stress test, it is responding to symptoms or risk factors that warrant this level of cardiac evaluation.
FAQs – Stress Tests
Q1. How long does a stress test take?
A: Exercise preparation and monitoring take 30–60 minutes. Nuclear or echo stress tests requiring additional imaging may take 3–4 hours total due to separate rest and stress imaging sessions.
Q2. Can I eat before a stress test?
A: Usually avoid eating for 2–4 hours before the test and avoid caffeine for 24 hours (caffeine affects adenosine-based pharmacological stress tests). Follow your clinic’s specific preparation instructions.
Q3. Is a stress test safe?
A: Exercise stress testing has an excellent safety record — serious complications (myocardial infarction, fatal arrhythmia) occur in approximately 1 in 10,000 tests. Testing is performed with continuous ECG monitoring, trained staff, and emergency resuscitation equipment immediately available.
Q4. What does a “positive” stress test mean?
A: A positive stress test suggests myocardial ischemia — insufficient blood flow to part of the heart during stress. It does not diagnose a specific coronary lesion but indicates that further evaluation (typically coronary CT angiography or cardiac catheterization) is warranted.
Q5. Does a negative stress test mean I have no heart disease?
A: A negative stress test significantly reduces the probability of significant obstructive coronary artery disease but does not entirely exclude it. The test has both false negative and false positive rates that depend on the test type, patient population, and pre-test probability of disease.